Thermographic Findings in Patients with Lumbar Spinal Stenosis Before and After Walking
Article information
Abstract
Objective
Patients with lumbar spinal stenosis experience a variety of symptoms, including back pain, and neurogenic claudication. However, these symptoms appear only after walking for a certain distance. Therefore, it is difficult to make an accurate diagnosis using conventional methods, which involve tests performed under resting conditions. Therefore, infrared thermography could be a helpful diagnostic tool.
Methods
Eight patients, who had neurogenic claudication after walking a certain distance, were enrolled in this study. These patients underwent infrared thermography at least twice after they walked a certain distance (about 50 meters after walking for 10 minutes). Four other patients, who only had back pain but no claudication, were enrolled as the comparison groups.
Results
Seven patients in the patient group showed a decrease of 0.6 to 2.3 degrees in body temperature, depending on the body regions evaluated, after walking a certain distance. However, in the comparison groups, only 1 patient had decreased body temperature after walking.
Conclusion
Neurogenic claudication symptoms are present in spinal stenosis patients because of venous congestion, which causes neurogenic claudication and decreases surface temperature. Therefore, infrared thermography can be performed in patients not only in resting conditions but also in symptom-expression conditions. Hence, infrared thermography can help in the accurate diagnosis of lumbar spinal stenosis.
INTRODUCTION
Patients with lumbar spinal stenosis complain of symptoms, such as back pain, lower extremity radiating pain, and neurogenic claudication. However, many patients have no distinguishing symptoms at resting state, but symptoms appear only after patients start walking for a certain distance. Therefore, it may be difficult to make an accurate diagnosis by using conventional methods, which are performed only under resting positions.
The skin is the largest organ in the human body, and the blood flow to the skin fluctuates. Skin function is influenced by several diseases, such as hypertension [3], genetic discordances of vascular reactivity [19], and peripheral vascular tone [13]. Skin temperature is affected by vasomotor activity, which is regulated by the peripheral sensory nerve fibers [6]. Infrared thermography has been used for the measurement of skin temperature in musculoskeletal disorders [4]. Particularly, infrared thermography is useful for the diagnosis and screening of neuropathy in patients with low back pain. The purpose of this study was to determine whether infrared thermography could be used to diagnose lumbar spinal stenosis through an analysis of changes in skin temperature after patients walk for a certain distance.
MATERIALS AND METHODS
A total of eight patients diagnosed with lumbar spinal stenosis were enrolled in this study. All patients complained of radiating pain, low back pain, or other symptoms (such as paresthesia) in resting conditions, and neurogenic claudication after walking for a certain distance. Patients with diabetes, heart disease, peripheral circulation disorders, or peripheral neuropathy were excluded in this study. For these patients, skin temperature was measured with infrared thermography. Thermographic tests were done at least twice for these patients, in resting state and in a condition when neurogenic claudication appeared after walking for a certain distance. The results were correlatively analyzed with the clinical symptoms of patients.
Other four patients were selected for the comparison groups. These four patients were divided two groups: one group included two patients who were very old and complained of only back pain; another group included other two patients who had no back pain. All of these four patients had neurogenic claudication after walking for a certain distance. The infrared thermography results were analyzed and compared in these groups.
RESULTS
Patients with spinal stenosis included 7 men and 1 women. The mean age at admission was 71.3 years, and ranged from 58 to 84 years (Table 1). All patients complained of neurogenic claudication after walking for a certain distance (about 50 meters after a 10-minute walk). Low back pain was present in 6 patients but not in the other 2 patients. Five patients presented with bilateral neurogenic claudication, and 3 patients had unilateral neurogenic claudication. The mean duration of symptoms was 16.8 months, and ranged from 3 months to 5 years.

Characteristics of 8 spinal stenosis patients who under-went infrared thermographic imaging
Seven individuals in the patient group showed a decrease of 0.6 to 2.3 degrees in body temperature, depending on the body regions examined, after walking for a certain distance (Fig. 1, Table 2). However, the extent of body temperature reduction was different in different individuals. In the comparison group, the body temperature increased by 1.5 to 5 degrees in the lumbar region and lower extremities in 2 patients, decreased in 1 patient, and did not change in another patient after 10 minutes of walking (Fig. 2). The alteration in skin temperature after walking was relatively consistent with the expression of symptoms, although quantitative analysis and comparisons were not performed in this study. No body temperature changes were observed in chronic low back pain patients who did not have neurogenic claudication.
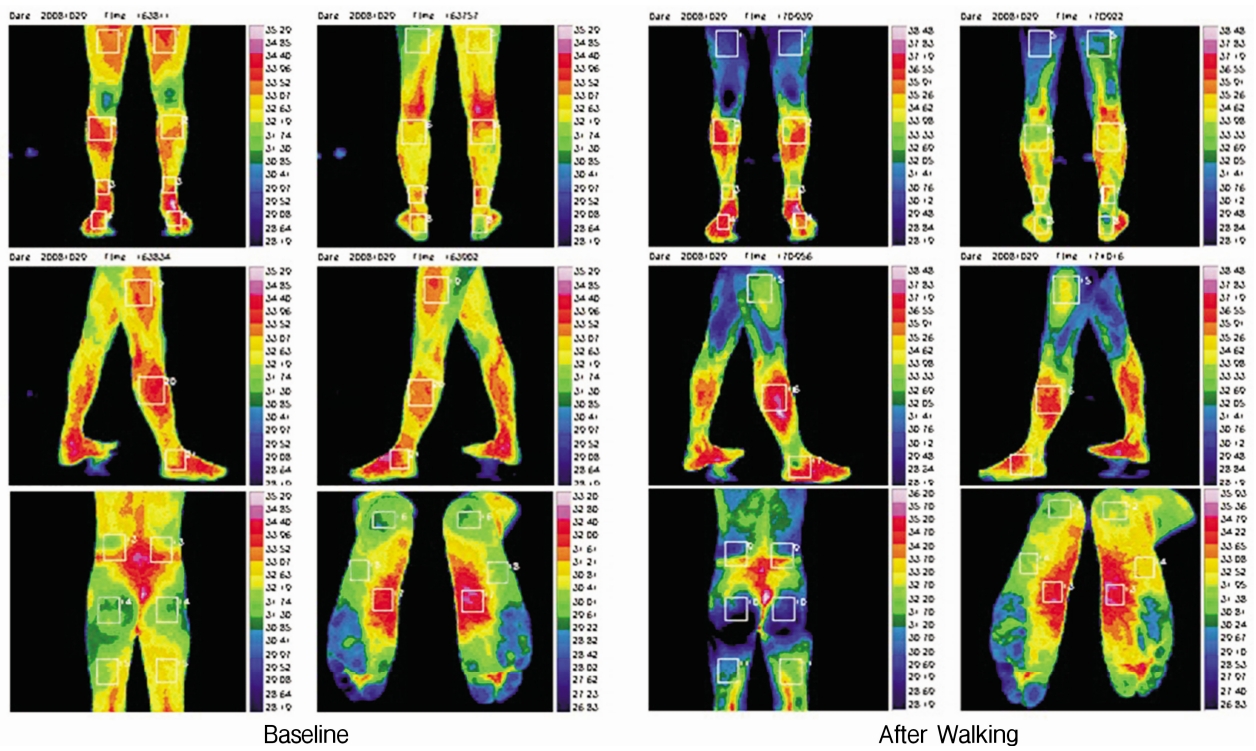
Comparison of thermographic images of a patient with lumbar stenosis and a symptom of claudication before and after walking.

Surface temperature changes in the patient and comparison groups

Comparison of thermographic images of a patient in comparison group before and after walking.
DISCUSSION
Claudication symptoms cause a decline in body surface temperature in regions affected by pain in patients with spinal stenosis. Neurogenic claudication symptoms occur in spinal stenosis patients because when the spinal root is compressed, venous congestion occurs, and the inadequate drainage reduces oxygenation or increases the accumulation of metabolites in the cauda equina [14]. Reduced oxygenation results in ischemia, which contributes to development of neurogenic claudication [2]. Transient ischemia often occurs during walking because of the increased oxygen demand [2]. Hypoxic ischemia can result in decreased surface body temperature [12]. Infrared thermography can promptly measure a decrease in skin temperature. Therefore, infrared thermography can be used to visualize the temperature changes that occur after claudication symptoms appear. Magnetic resonance imaging (MRI) can be used to visualize static symptoms in patients under resting conditions, but infrared thermography can reveal dynamic changes in patients in a convenient manner.
Patients with lumbar spinal stenosis show several symptoms, such as low back pain, lower extremity radiating pain, and claudication. However, these symptoms sometimes do not appear under resting conditions and can be observed only after the patients walk for a certain distance. Therefore, it is difficult to make an accurate diagnosis using conventional methods, which involve tests that are performed only under resting conditions.
The skin surface radiates infrared rays in a wavelength range of 900-14,000 nanometers, and infrared thermography can be used to detect this infrared radiation. Subsequently, infrared thermography can be used to produce a visible two-dimensional image of the distribution of the skin surface temperatures of the human body [20]. Infrared thermography was first used in the medical field in 1956 [10]. Thereafter, many related studies have been performed in several fields, such as mammology, rheumatology, orthopedics, neurology, and vascular imaging, and for different types of screenings or physiological response examinations [8,15]. Infrared thermography, suitable for objective visualization of skin temperature, is a valuable and non-invasive technique for diagnosis. The pathological examination of spinal stenosis is another potential use of infrared thermography. Abert et al. [1] first used infrared thermography to measure skin temperature in low back pain patients. Subsequently, several related reports have been published. For example, some studies used a highly sensitive infrared thermography protocol to show that skin temperature abnormalities were associated with spinal radiculopathy [5,9,16-18]. The findings confirm that the results obtained using infrared thermography are well correlated with those obtained with computerized tomography (CT), myelography, and MRI. Moreover, Hakelius et al. [7] and Lindholm et al. [11] commented that low temperature measured in the lower extremities indicated the possibility of spinal nerve root compression.
Symptoms do not explicitly appear in many cases of lumbar spinal stenosis. CT or MRI is performed under resting conditions, where the symptoms are not present; therefore, it is difficult to correlate the patient`s symptoms with the findings obtained with CT or MRI. Moreover, it is also difficult to choose a treatment plan with the results from other medical techniques, such as electromyography and examination of somatosensory evoked potentials. In this study, we could directly identify actual lesions using infrared thermography by measuring changes in body temperature when the patient’s symptoms appeared. Infrared thermography can help in designing a detailed treatment plan based on the identification of the actual lesions, which are difficult to detect using CT or MRI alone. Another feature of infrared thermography is that the therapeutic effects can be easily observed. Currently, we are examining the effect of treatment by investigating the changes in subjective symptoms after conservative treatments, such as Nerve block, radiofrequency ablation, or surgery. Through a comparison of the results obtained before and after surgery using infrared thermography, objective conclusions regarding the effects of the surgery can be obtained. The symptoms that patients complain are the most important indicator for the diagnosis but more advanced diagnosis techniques are needed for the management of patients.
Our study has several limitations. First, the number of patients was too small to perform statistical analyses. Second, infrared thermography before walking was performed in a standardized environment, but infrared thermography after walking was done not in stable position. Therefore, the test conditions before and after walking were different.
CONCLUSION
In this study, infrared thermography was used to measure skin temperature in patients, not only under resting conditions but also under conditions where symptoms appear. Infrared thermography can help in the accurate diagnosis of lumbar spinal stenosis. However, further studies are needed in order to determine the practical usefulness of infrared thermography, to reveal correlations between the severity of symptoms and body temperature, and to standardize the test conditions.