Cervical Spondylodiscitis with Neurologic Deterioration after Percutaneous Cervical Nucleoplasty
Article information
Abstract
Percutaneous cervical nucleoplasty (PCN) has proven to be a safe and effective technique for the management of the cervical herniated or bulging discs. The incidence of cervical spondylodicitis (CSD) after PCN is rare. Case 1: A 53-year-old male patient was admitted with right arm motor weakness, severe posterior neck pain. He diagnosed with a C5-6 bulging disc and underwent a PCN two months prior to admission to our hospital. Laboratory tests revealed WBC counts and CRP levels, but his erythrocyte ESR was mildly elevated to 42 mm/hr. MRI showed a CSD at the C5-6 level. The patient underwent an anterior cervical C5 corpectomy and fusion. A microbiological culture revealed the presence of Propionibacterium acnes. Case 2: A 51-year-old female patient was admitted with quadriparesis. She was diagnosed with a C6-7 bulging disc and underwent a PCN two weeks prior to admission to our hospital. Laboratory tests revealed and elevated WBC count of 13.1×103/mm3, elevated ESR of 70 mm/hr, and elevated CRP of 10.1 mg/dL. The MRI showed a high signal intensity around the C5-6 vertebral body and epidural fluid collection on the axial image. The patient underwent a C6-7 anterior cervical discectomy and. No microbes were identified in blood or pus cultures. Clinicians should consider CSD, if a patient’s neurologic symptoms have deteriorated within 8 weeks after PCN. If clinical and laboratory tests show any indication of CSD, MRI should be performed facilitating appropriately timed treatment in order to prevent neurological sequelae.
INTRODUCTION
Percutaneous cervical nucleoplasty (PCN) has proven to be a safe and effective technique for the management of cervical herniated or bulging discs, with a 70-90% postoperative efficacy rate7 [8,15],. Although several PCN-related complications have been reported, intervertebral discitis most frequently occurs following PCN and the incidence varies between 1.8-5.3% [2,5]. Cervical spondylodiscitis (CSD) is thought to be preceded by discitis with an even lower incidence rate [13]. Despite being uncommon, discitis and epidural abscess in the cervical region have been reported to have a relatively higher mortality rate of 21%, compared to the 3.6% with those involving the thoracic and lumbar regions [14]. It is important to diagnose CSD early and to treat them appropriately. However, if the surgeon excessively coagulates the disc or damages the endplate during PCN, it is difficult to distinguish CSD from spondylitis or simple discitisrelated postoperative changes. As a result, the optimal time window to treat CSD can be missed. Additionally, controversies exist regarding the appropriate CSD treatment methods.
Herein we discuss two patients who presented with CSD after PCN at a local hospital. One patient underwent an anterior cervical C5 corpectomy and fusion using an autologous iliac bone graft with C4-6 plate fixation, and one patient underwent a C6-7 anterior cervical discectomy and fusion (ACDF) using an autologous iliac bone graft with plate fixation.
CASE REPORT
Case 1
A 53-year-old male patient was admitted to our hospital with right arm motor weakness, severe posterior neck pain, and right arm radiating pain. He had chronic myelogenous leukemia (CML) as an underlying disease. He visited a local hospital with posterior neck pain and was diagnosed with a C5-6 bulging disc and underwent a PCN two months prior to admission to our hospital. After the procedure, the patient’s posterior neck pain did not improve and he was treated with non-steroidal anti-inflammatory drugs (NSAIDs) for 2 weeks. However, the patient’s symptoms gradually worsened. Physical examination showed right arm motor weakness: right elbow flexion grade IV, wrist extension grade IV, elbow extension grade IV, and hand grasp grade III. The hypoesthesia was observed in the C6 sensory dermatome. Laboratory tests revealed normal white blood cell (WBC) counts, and C-reactive protein (CRP) levels, but his erythrocyte sedimentation rate (ESR) was mildly elevated to 42 mm/hr (normal range: 0-20mm/hr). He had no fever or chills at the time of admission. A simple cervical spine X-ray showed an osteolytic C5-6 lesion, retrolisthesis of C5 on C6, and thickening of prevertebral soft tissue (Fig. 1A). T1-weighted magnetic reso nance imaging (MRI) showed low signal intensity in the C5-6 vertebral body (Fig. 1B). A contrast-enhanced MRI showed enhancement of the C5-6 vertebral body and right-side epidural fluid collection (Fig. 1C, D). Based on the physical examination and radiologic findings, he was diagnosed with CSD at the C5-6 level and we decided to perform surgery.
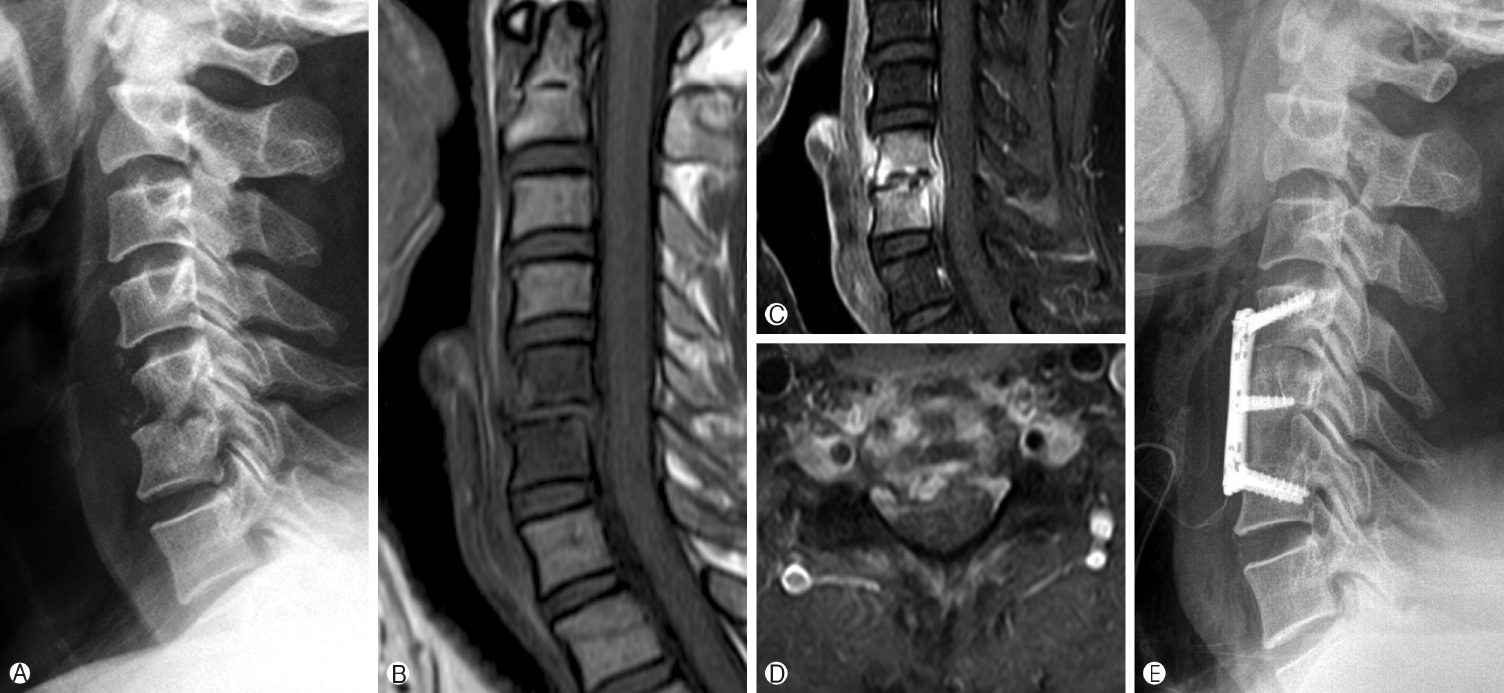
(A) Simple cervical spine X-ray showing an osteolytic lesion at C 5-6, retrolisthesis of C5 on C6, and thickening of prevertebral soft tissue. (B) A T1-weighted MRI showing low signal intensity in the C5-6 vertebral body. (C, D) A contrast-enhanced MRI showing enhancement of the C5-6 vertebral body and right-side epidural fluid collection. (E) A postoperative simple cervical spine X-ray showing the C5 corpectomy and fusion using an autologous iliac bone graft with C4-6 plate fixation.
Intra-operatively, the C5-6 disc was destructed, and granulation tissue with a small amount of dark colored pus was observed. A C5 corpectomy was performed with removal and cleaning of the abscess following collection for culture and biopsy. Afterwards, an autologous iliac bone graft with an anterior titanium cervical internal fixation was performed (Fig. 1E). A microbiological culture revealed Propionibacterium acnes with sensitivity to ceftriaxone, which was immediately administered. The patient’s symptoms gradually improved, and he was discharged without neurological symptoms.
Case 2
Intra-operatively, the C5-6 disc was destructed, and granulation tissue with a small amount of dark colored pus was observed. A C5 corpectomy was performed with removal and cleaning of the abscess following collection for culture and biopsy. Afterwards, an autologous iliac bone graft with an anterior titanium cervical internal fixation was performed (Fig. 1E). A microbiological culture revealed Propionibacterium acnes with sensitivity to ceftriaxone, which was immediately administered. The patient’s symptoms gradually improved, and he was discharged without neurological symptoms.A 51-year-old female patient was admitted to our hospital with quadriparesis. She had no underlying disease. She visited a local hospital with radiating pain in both arms, and was diag nosed with a C6-7 bulging disc, and underwent PCN two weeks prior to admission to our hospital. After the procedure, the patient’s symptoms gradually worsened leading to paralysis. In the local hospital, the clinicians managed the patient with NSAIDs and, as the patient’s symptoms deteriorated, serial follow-up MRIs were performed 1 and 2 weeks after the PCN(Fig. 2). A pre-operative T2-weighted MRI showed a C6-7 mild bulging disc (Fig. 2A). A T2-weighted MRI 1 week after the PCN showed a mildly high signal intensity around the C5-6 vertebral body (Fig. 2B). A T2-weighted MRI 2 weeks after the PCN showed an increased high signal intensity around the C5-6 vertebral body and epidural fluid collection on the axial image (Fig. 2C). There was no contrast enhanced MRI image from the local hospital. Her WBC count, ESR, and CRP levels 4 days after the PCN were 10.6×103/mm3 (normal range: 4.8-10.8×1103/mm3), 35 mm/hr (normal range: 0-20 mm/hr), and 11.03 mg/dL (normal range: 0-0.3 mg/dL), respectively. One week after the PCN, her WBC count, ESR, and CRP level were 11.6×103/mm3, 38 mm/hr, and 6.90 mg/dL, respectively, in the local hospital laboratory testing.
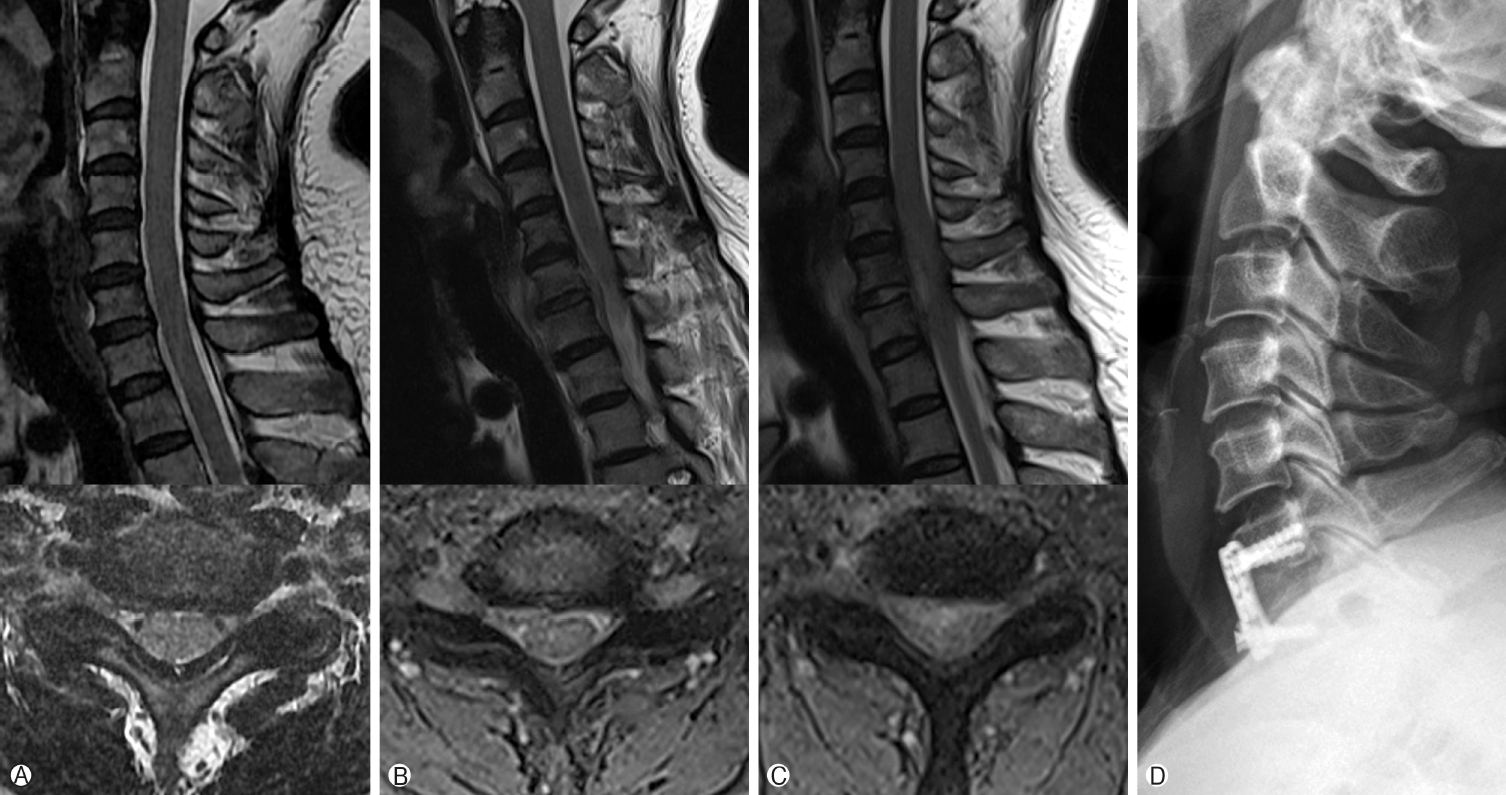
(A) A pre-operative T2-weighted MRI showing a C6-7 mild bulging disc. (B) A T2-weighted MRI 1 week after PCN showing a mild high signal intensity around the C5-6 vertebral body. (C) A T2-weighted MRI 2 weeks after PCN showing an increased high signal intensity around the C5-6 vertebral body and epidural fluid collection in the axial image. (D) Postoperative simple cervical spine X-ray showing a C6-7 ACDF using an autologous iliac bone graft with a C6-7 plate fixation.
When the patient was admitted to our hospital, physical examination showed both arm and leg motor weakness. The hypoesthesia was observed in the C5-6-7 sensory dermatome. Laboratory tests revealed that her WBC count had increased to 13.1 ×103/mm3, ESR was elevated to 70mm/hr, and CRP level had increased to 10.1 mg/dL. However, she had no fever or chills at the time of admission. Based on the physical examination and radiologic findings at the local hospital, we diagnosed with CSD at the C6-7 level and decided to perform surgery.
Intra-operatively, yellowish pus was observed at the posterior side of the disc. A C6-7 discectomy was performed with removal and cleaning of the abscess following collection for culture and biopsy. Afterwards, an autologous iliac bone graft with an anterior titanium cervical internal fixation was performed (Fig. 2D). After surgery, the patient’s neurological symptoms gradually improved. Even though no microbes were identified in the blood and pus cultures, we decided to continue vancomycin treatment for 8 weeks. Finally, the patient was discharged without neurological symptoms and with a normal WBC count, ESR, and CRP level.
DISCUSSION
Ablation and coagulation are key PCN techniques for decompression the disc with minimal damage to the surrounding skeletal structures [12]. PCN has several advantages compared to ACDF and total disc replacement, such as shorter operative times, fewer complications, and shorter hospital stays due to the use of local anesthesia and percutaneous techniques [10]. Until now, PCN has proven to be a safe and effective treatment modality for management of cervical herniated or bulging discs, with 70-90% postoperative efficacy rates [7,8,15]. Due to these reasons and the excellent outcomes and safety of PCN, initial surgical treatments for cervical degenerative disc disease have steadily shifted away from ACDF and towards PCN. Although several PCN-related complications have been reported, such as intervertebral discitis, broken device tips, and postoperative hematoma, the complication rate is very low [3]. Among them, the incidence of intervertebral discitis is 1.8-5.3% [2,5] and that of CSD, which is thought to be preceded by discitis, is even rarer [13]. However, despite being uncommon, CSD has been reported to have a relatively higher mortality rate of 21%, compared to the 3.6% with those involving the thoracic and lumbar regions [14]. In addition, if the surgeon coagulates the disc excessively or damages the endplate during the PCN, it is difficult to distinguish CSD from spondylitis or simple discitis-related postoperative changes. As a result, the optimal time window to treat CSD can be missed leading to irreversible neurological deficiencies. In our cases, the clinicians at the local hospital might have diagnosed postoperative symptoms as simple discitis and managed patients with NSAIDs only.
It is important to diagnose CSD early and to treat them appropriately. In order that, clinicians should understand the natural course of postoperative CSD. According to previous reports, the patients’ symptoms of postoperative CSD did not improve and became aggravated after surgery, with the development of new neurological symptoms within 4 to 8 weeks [1,9]. Fever is also a typical symptom. In our cases, posterior neck pain was aggravated, and new neurological symptoms appeared within 8 weeks after the PCN, but the patients did not present with fever. Among laboratory findings, the ESR and CRP level are regarded as sensitive and specific screening tools for infection at 100% and 95.8%, respectively [12]. However, during the early postoperative period, the ESR and CRP levels may increase as a result of tissue damage caused by the surgical procedure itself. Furthermore, Lee et al. [9] reported a CSD case after PCN without abnormal laboratory findings within 8 weeks. They also reported it to be related to minimal invasiveness of PCN. In our first case, it was difficult to screen for infections with laboratory tests, because the patient had CML as an underlying disease. In our second case, the patient’s postoperative laboratory findings were shown to be improving over time in the local hospital. To screen for postoperative infections after minimally invasive procedures with laboratory testing, further evaluations are needed to clarify the changes in inflammatory markers. In addition, we suggest that clinicians should consider the possibility of a CSD if a patient’s neurological symptoms deteriorate within 8 weeks after a PCN with normal laboratory findings.
With widespread access and advances in neuroimaging techniques, MRIs are the gold standard for diagnosing spondylodiscitis. An MRI is considered to be the most sensitive (93%) and specific (97%) diagnostic tool for spondylodiscitis [6,11]. If there are any indications for CSD in clinical and laboratory results, an MRI should be performed for an accurate diagnosis. When CSD is diagnosed, surgical or medical treatments should be considered. If there are no neurological symptoms or structural instabilities, it is recommended that the correct antibiotic therapy by given to patients following disc biopsy for identified microbes [4]. If there are pathological fractures, neurological deficits, and epidural abscess formations with CSD, a complete debridement of the disc space, posterior longitudinal ligament, and devastated bony endplate should be performed as in our cases [16]. Subsequently, it is important to reconstruct the cervical spinal alignment. Autologous iliac bone graft is the most favorable grafting source and internal instrumentation is necessary to ensure immobilization. The goal of surgery is not only restoration of the alignment, but also to identify any microbes for further antibiotic treatment.
CONCLUSION
Clinicians should consider CSD if a patient’s neurological symptoms deteriorate within 8 weeks after a PCN. Further, inflammatory markers such as WBC count, ESR, and CRP level should be carefully checked even after minimally invasive procedures. If there are any indications of CSD in clinical and laboratory results, an MRI should be performed facilitating appropriately timed treatment in order to prevent neurological sequelae. In addition, surgical decompression and fusion should be considered as the first treatment option for CSD with neurological deficits, which could achieve the restoration of the cervical spinal alignment and the identification of microbes allowing for the selection of appropriate antibiotics.
Notes
All authors associated with this submission have no financial conflicts of interest to disclose.
Abbreviations list
PCN
Percutaneous cervical nucleoplasty
CSD
Cervical spondylodicitis
WBC
White blood cell
CRP
C-reactive protein
ESR
Erythrocyte sedimentation rate
MRI
Magnetic resonance imaging
ACDF
Anterior cervical discectomy and fusion
CML
Chronic myelogenous leukemia
NSAIDs
Non-steroidal anti-inflammatory drugs